On March 27, 2024 Carlos Quinonez was the speaker at the Royal College of Dentists of Canada (RCDC) webinar. Below is the transcript (word for word, including misspoken words) of that meeting including the slides used.
The Royal College of Dentists of Canada (RCDC) is a regulatory college which administers examinations for qualified dental specialists as part of the dental profession in Canada.
TRANSCRIPT of the RCDC Webinar on CDCP
Okay, I think that’s adequate. Thank you, Karine. So it gives me great pleasure to introduce tonight’s moderator. Dr. Sonika Singhal is moderating tonight’s session. She’s an RCDC fellow in dental public health.
She’s a dental public health specialist with a bachelor’s degree in dental surgery from Delhi University in India, Masters in Public Health from the University of New South Wales, Australia, and a combined degree specialty in dental public health and PhD in Dentistry from the University of Toronto.
She is the program director, dental public health discipline at the Faculty of Dentistry at the University of Toronto. Sonika, good evening and thank you for volunteering your time to moderate tonight’s session.
The floor is all yours.
Thank you. Thank you, Dr. Czar, for the introduction. And good evening, everyone. It’s my utmost pleasure to be here today for moderating this session and introducing Dr. Carlos Quinones. I’m sure a lot of people already know him so well, but for those who are new to RCDC, Dr.
Quinones is a dental public health specialist, RCDC fellow, and he had been program director for dental public health discipline at the University of Toronto for the longest time before he moved to Western in 2022.
And there he’s vice dean and director of dentistry at Schule School of Medicine and Dentistry. I would also like to share that he was my PhD supervisor and he held my hand to help me in making baby steps in the discipline of dental public health.
So on that note, I will say he is a great educator and a mentor. And I’m glad that we are hearing all about CDCP and in dental care plan from him. So on that note, I introduce Carlos. The floor is all yours.
Thank you.
Thank you, Sonica, and you always make me cry when you talk like that, so. All right, so thank you, everybody, for for coming today. I couldn’t be more thankful for your time this evening. I’m sure you have many other things to do, but you’ve taken the time to come listen to this, so thank you very much.
I want to say that these ideas are still not completely concrete in my head, so they’re a bit of a work in process, so I encourage you to email me and tell me where you think I may be wrong or where I can maybe clarify my arguments.
So nonetheless, a work in progress, but I do think an important topic for us to consider. So let me see here. Okay, so I’ll begin with declaring a conflict of interest. So I’m going to read this, that due to the positions I’ve held in my specific expertise, I have been a regular consultant to public and private agencies regarding issues of dental care policy and practice.
I have consistently expressed my opinions and recommendations based on the evidence that was present at the time I was consulted. Some of the data presented here may have been funded or partially funded by agencies that may be mentioned in this presentation.
Confidentiality agreements may not allow me to mention specific agencies by name or answer certain questions.

So with that said, we are clearly in a time of change. The Federal Dental Care Plan is the single most consequential public policy intervention in the last 40 to 50 years.
It has highlighted a complex set of interrelated public policy issues for us in our profession that I believe require attention from all stakeholders. One could say that we are potentially reaching an inflection point in dentistry, and hopefully what I talk about tonight will help you understand why I may think that.
I’ll start off by telling you that when all of this started, I was invited to an in -camera meeting of Canada’s most influential scholars and thought leaders in constitutional law, public administration, health law, health care history, health care policy, and health economics.
I felt very lucky to be there given the level of intellect and experience in the room, and I wondered why they would be interested in this topic. Well, to some extent, it could be that dental care has gone international.
The World Health Organization, the United Nations, the World Dental Federation have all essentially doubled down on the idea of including dental care within universal health care coverage. Really, they want to answer the question, or we’re thinking about answering the question, how best to deal with dentistry within broader health care policy.
And I think it’s very important for dentists to understand that we are now part of much larger policy agendas. This is no longer about your province or even our country. This is about international movements with respect to health care and health care policy.
And one of the things that caught me by surprise is that one of Canada’s leading health care economists said this during the meeting, that dentistry is a classical example of a market failure and is ripe for policy intervention.
Now, I’m not going to unpack that. I’m not even going to say whether I agree with it or not, but I think it gives you a sense of where we might be today.
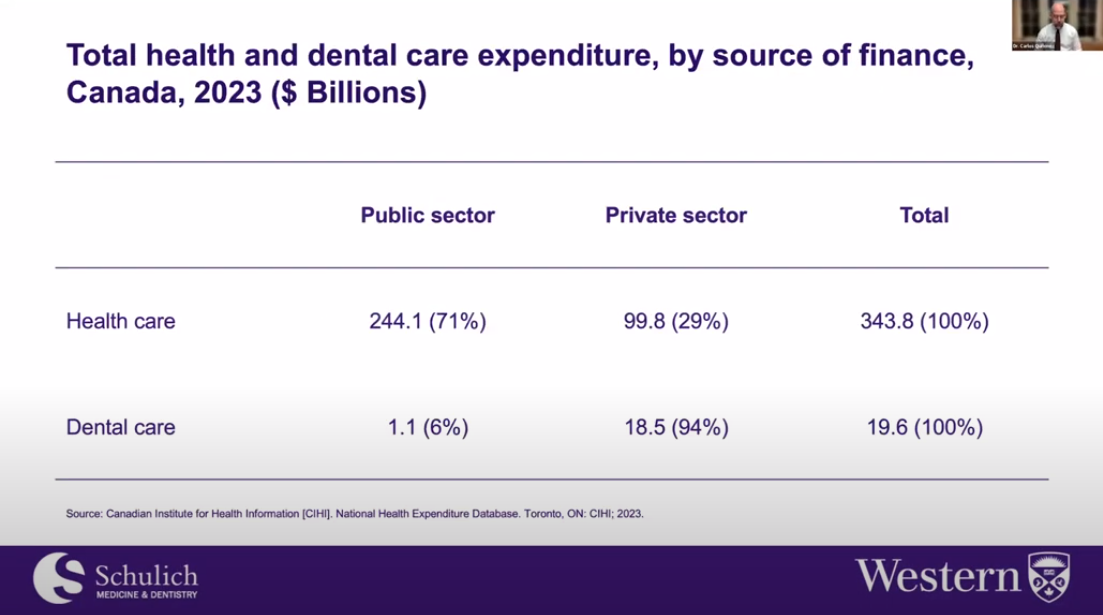
So let’s first orient ourselves. How do we spend money now with respect to health and dental care?
And as you can see, 71% of health care spending, at least in 2023, was from the public sector and the remainder, 29% was privately funded. This includes things like dentistry, pharmacy service, and so on.
Now, if you look at dentistry, the great majority of that, 94% is funded privately, as many of you are well aware, and only 6% is funded publicly by different levels of government. So how do we rank internationally?
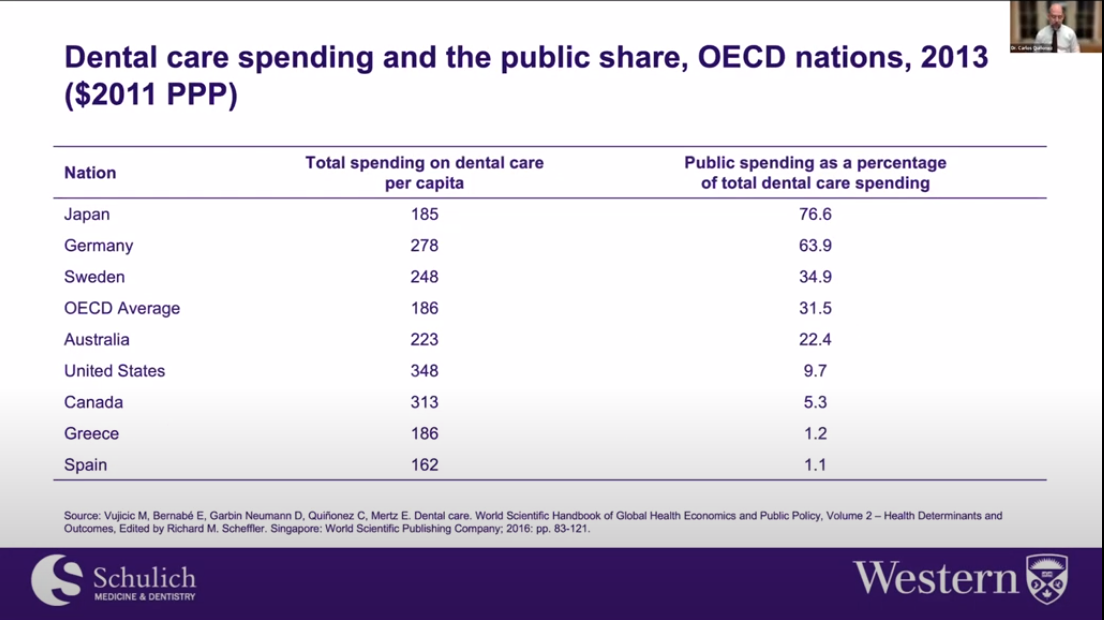
Again, I don’t need you to look at these numbers in great detail, but just to tell you that we are far behind the OECD average with respect to the amount of money that governments invest in dental care compared to places like Japan, Germany, and Sweden.
And in fact, with the funding provided by the federal dental care plan, we will come much closer instead of about five to 6%. We will be closer to about, let’s just say 27% to 28% depending on how much money is spent.
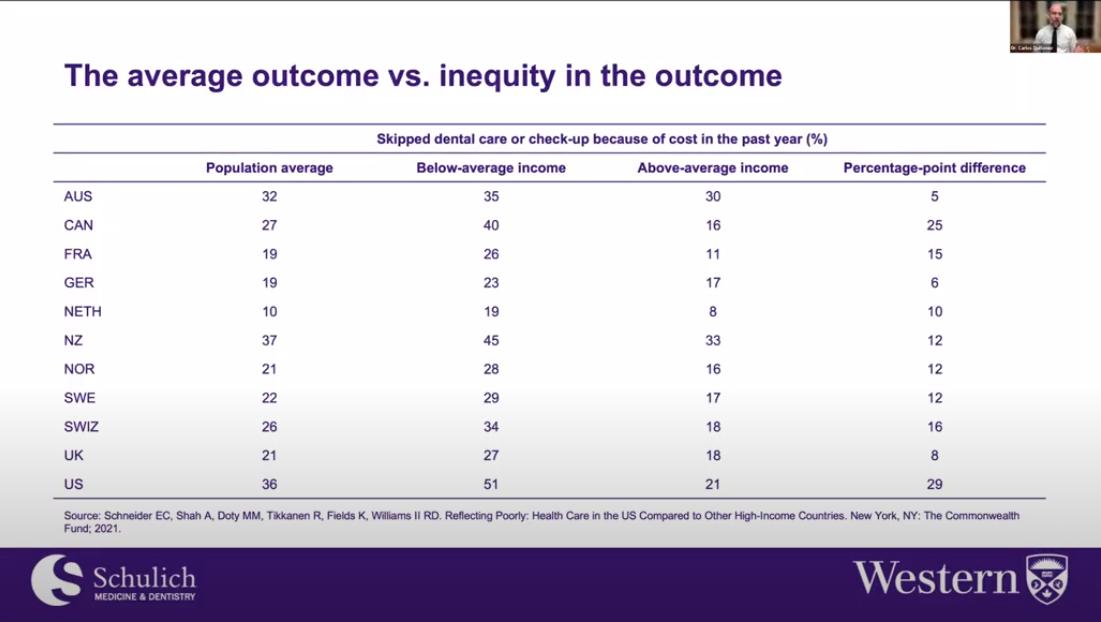
So what are the consequences of such small amounts of public investments in dental care? Well, again, don’t worry about all these numbers, but just to say that on average, about 27% of Canadians report skipping dental care or a checkup because of the cost in the past year.
And we don’t do too well here. We’re kind of in the lower third of OECD nations, or in this case, Commonwealth nations. But where you really see the stark issues at play is when you compare people with below average incomes with people with above average incomes.
And here we are only second to the United States with respect to these countries in terms of that difference with respect to skipping dental care because of costs. So really such low levels of public investments has resulted in quite an inequitable dental care system.
And this is exactly the public policy issue that the federal government in part is trying to address.
So where have we been? Well, I like to think lots about the history of dentistry. So I wanna give you a sense of how it is that we got here.
I of course like to concentrate on the long game because ultimately in public policy matters, it is the long game that matters. In fact, I would argue that we could have foreseen the federal dental care plan and could have prepared much more effectively as a profession.
And even as some wish, I would go as far as to argue that we could have staved off such public policy intervention. So let me take it back to 1938, the Royal Commission on Dominion Provincial Relations.
We don’t need to spend a lot of time here, but it was just a Royal Commission task with thinking through how the federal government was gonna work with the provincial governments and vice versa, how we were gonna share tax revenues.
And part of that discussion was thinking about including or developing a national system of health insurance. We never got one at this stage. But it was a discussion about medicine, hospitals, dentistry, nursing, and so on.
Then we moved to the Hospital Insurance and Diagnostic Services Act, which was really the first major step in building our Canadian healthcare system. And HIDSA, as it is called, was celebrated as a major achievement, not only for nationalizing hospital care and removing cost barriers to that care, but also as a great advancement in federal provincial relations.
Then comes the Royal Commission on Health Services, which was really the commission that structured our healthcare system as we know it today. It brought in physician services and to the already nationalized hospital services.
Now it didn’t include dentistry. There’s some really interesting reasons for that. We won’t get into that today. But nonetheless, this is where we get Medicare. Several years later, we get the Medical Care Act at the federal level, which again, structures our Medicare system as we know it today.
Now for dentistry, we were included in something called the Canada Assistance Plan, which was a way for the federal government to flow money into the provinces for things like dental care for people on social assistance, low -income children, the things that we know happen in quote unquote public dentistry today.
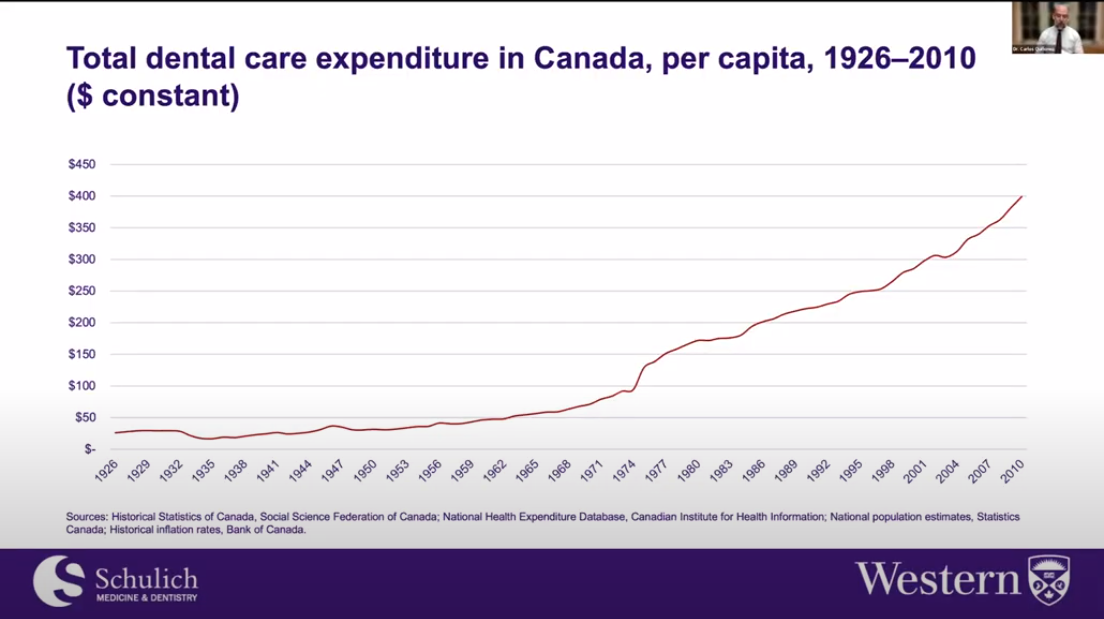
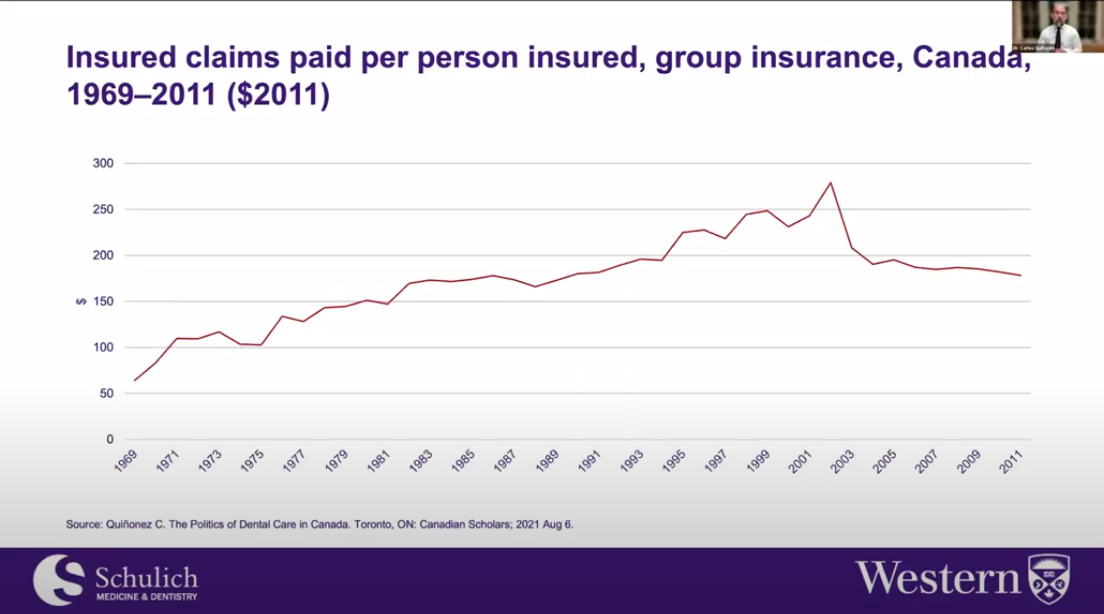
This significant bolus of funding for dental care expenditures in Canada is really the result of not public funding but of the fact that private insurance began to take hold in Canada and really gave rise to the employer -sponsored dental benefits that we know today.
And we’ve, to some extent, we’ve been spending more and more money on dental care in Canada since that time.
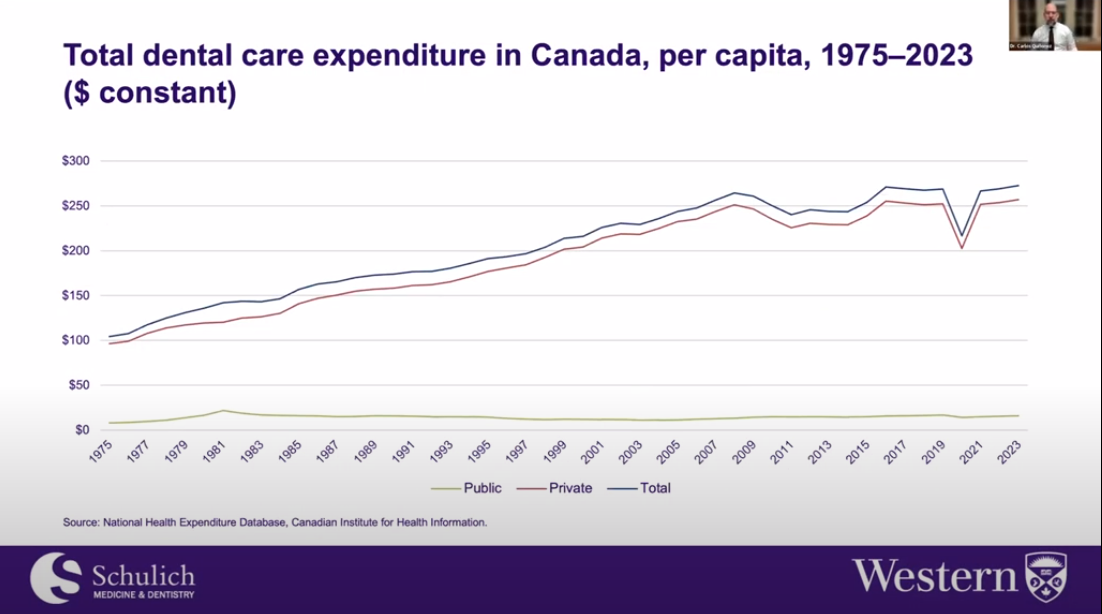
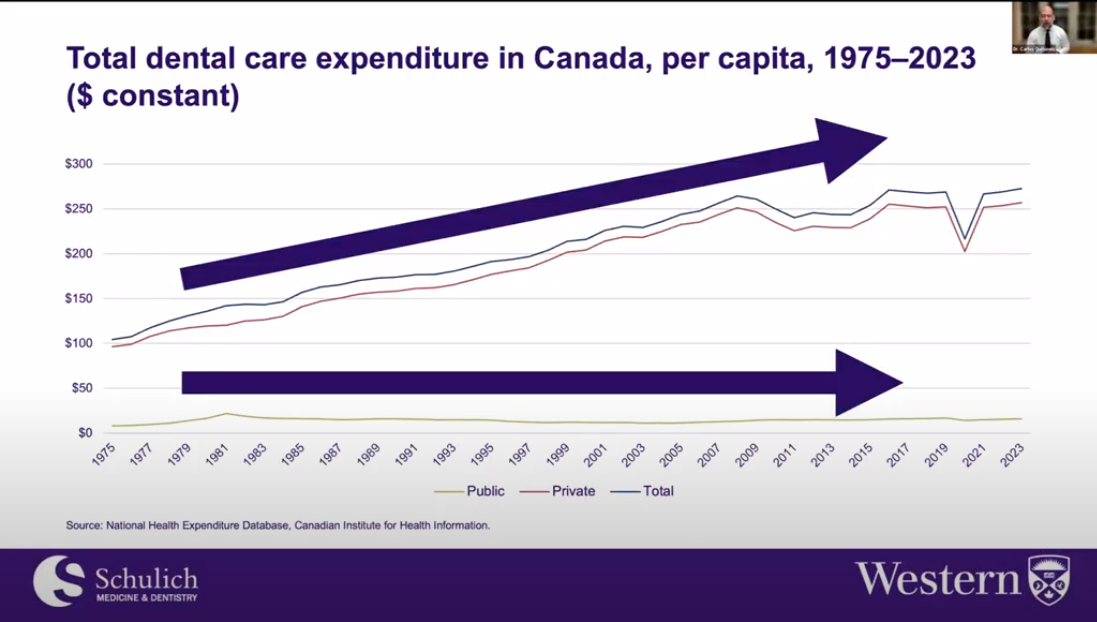
Now let’s look at the same expenditure curve but now brought up to 2023 again in constant dollars meaning we’re controlling for inflation.
We’ve also disaggregated this curve so that we see the red line which is private expenditure. So obviously we fund most things privately in dentistry because it tracks along the blue line which is total expenditure and the green line is public.
So again we’ve been on this upper trajectory and this is I wouldn’t say unheard of but you know dentistry has been very lucky in terms of society’s investments in it at least from a private perspective.
The economic crisis or the financial crisis of 2008 -2009 took a big chunk out of dentistry but we rebounded and here you can see the effects of COVID -19. I’d like you to notice so that we’re maybe not on as steep a trajectory as we have been in the past and we may be leveling out and I think there are reasons for that that we will review shortly.
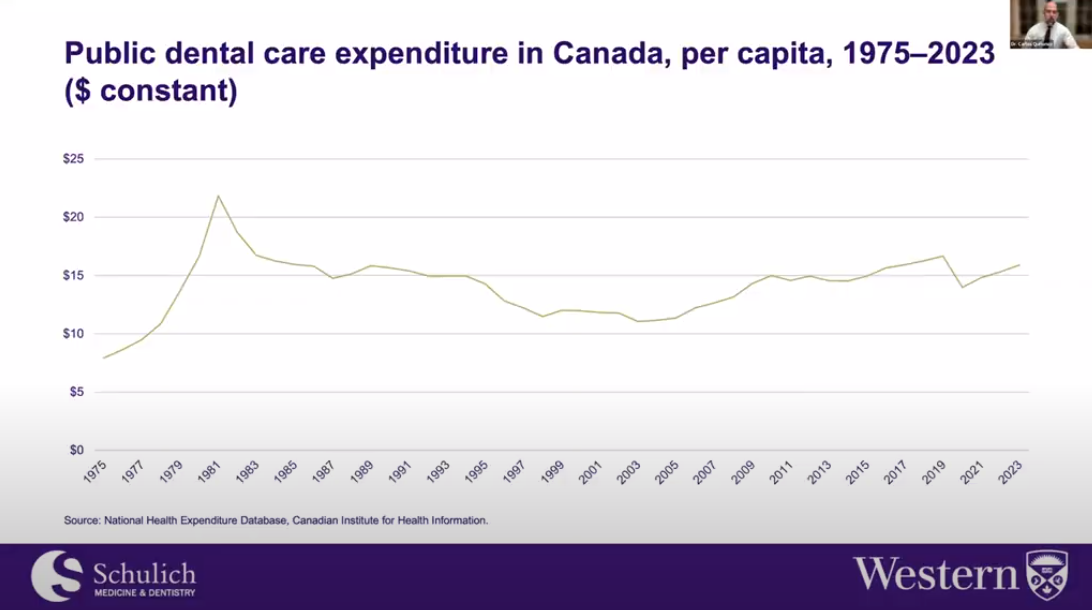
Now let’s look at what is happening publicly. If we zoom in on public expenditure here we can see the major investments that were made for public dental care plans by governments throughout the 60s, 70s.
They tended to trail off in the early 80s because of a recession and at this point we were about 20 percent public expenditure out of all dental care expenditure compared to where we are now you know four to six percent now and again with the federal dental care expenditure we will we will reach closer to 80 sorry 30 percent closer to the OECD average.
Again we reached an inflection point in the early 80s and we’ve seen nothing but declines up until the early 2000s what is what is known in the literature as welfare state retrenchment or this idea that the state is moving away from these types of public programs and this was very very difficult for public dental care programs but we’ve seen some a bit of a rebound.
Well why might that be? Well the Canadian Dental Association in the rural commit non -rural commission part of me the future the Commission on the Future of Healthcare in Canada or the Roman Oak Commission provided advice and along with other professional groups like the Canadian Dental Hygienist Association the Canadian Association of Public Health Dentistry and others argued that we needed to make reinvestments in dentistry and one of the outcomes of that was the creation of a new Chief Dental Office Chief Dental Officer position at the federal level and I was lucky enough to be Dr.
Peter Cooney’s first first intern and he was not the first Chief Dental Officer we’ve had in Canada but definitely the first one and I would call them our modern era and but it didn’t stop there. British Columbia made investments, Alberta made investments, Manitoba made investments, Newfoundland and Labrador made investments, Saskatchewan, Ontario, Quebec, Saskatchewan again, Ontario again, PEI very recently, the Yukon most recently.
So what I’m giving you a sense of is that you know the federal dental care plan is not something that appears out of nowhere. It’s part of a 15 to 20 year trajectory of governments feeling that they need to get involved more in dentistry to address a variety of issues and I’ve highlighted the issue of inequity and being able to access dental care and it just wasn’t the Canadian Dental Association and other dental groups making public policy statements.
Here we see the Canadian Pediatric Society talking about a call to action for children around oral health care, a left -leaning think tank, the Canadian Centre for Policy Alternatives weighing in. putting our money where our mouth is, the future of dental care in Canada, Canada’s most celebrated academics weighing in, in terms of access to oral health care for people, for vulnerable people living in Canada, a right leaning think tank, talking about equity and efficiency in Canada’s dental care system.
That in itself should be a major, major signal to us that maybe the ship isn’t moving as well as we think it might be. The emergency physicians stepping in, saying that we’re having unnecessary impacts on the healthcare system because of people’s inability to access dental care, the Canadian Dental Association itself.
This is a wonderful report if you get a chance to look at it at a time to reinvent ourselves in Canadian dentistry in order to stave off some of the things that we feel we are fighting today, for example, with the new federal dental care plan.
Eventually, the need for something like this being mentioned in the throne speech at the federal level, and then ultimately legislation for the first stage of this new public policy intervention federally, being the Canada Dental Benefit for children, which was a direct cash transfer to families in order to access dental care.
And then ultimately we are here today with the idea of whether Canada should have a much robust intervention with respect to dental care. And then obviously the answer is yes. So a lot of open questions remain.
A lot of things remain to be answered. But nonetheless, we are moving to where international health policy agendas say we should be moving to, which is more investments from governments in dental care or thinking about how to push dental care, not wholly, not completely, but at some level into a universal health care package.
And again, the broader public policy question is how best might we deal with dental care within broader health care policy?
Pardon me here. So let me just go back. I wanna show you this expenditure curve again, just to show you that there’s an inherent tension in what we’ve been doing in Canadian dentistry for the past 20 to 40 years, meaning we’ve been spending more and more money on private dentistry and spending less and less money, regardless of a little bit of a rebound over the last little while with respect to public dentistry.
This has created a significant tension in our profession and anybody who’s paying attention from a public policy perspective. And this tension is very generative. It’s resulting in a lot of change. I can show you that tension through images like this.
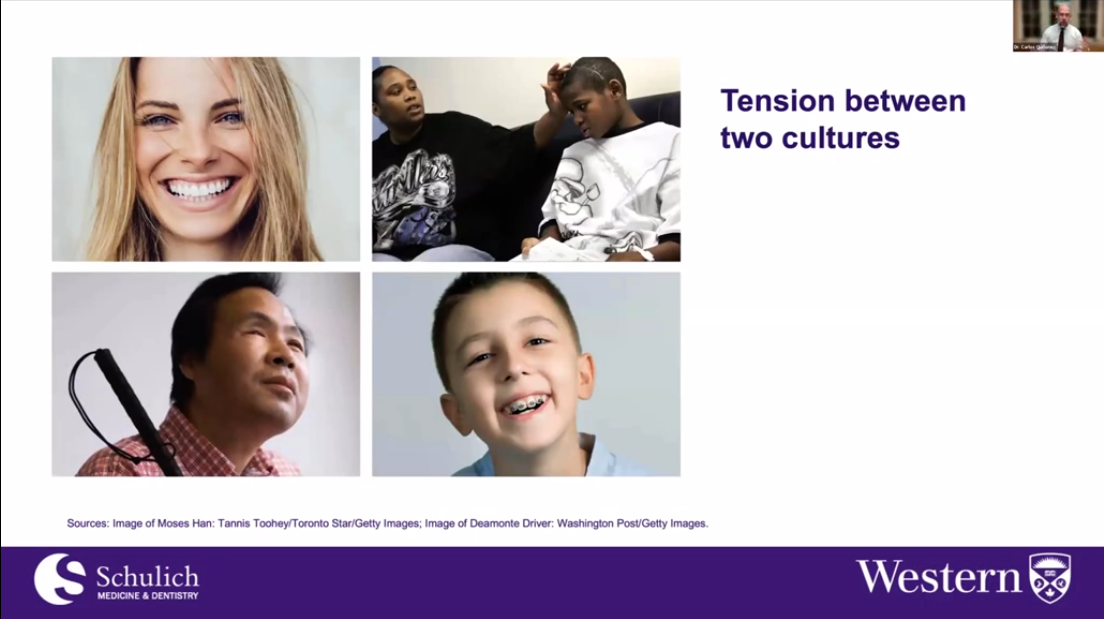
Straight white teeth is linked to health and wellness, but then we have people that fall through the cracks and ultimately suffer. Some people suffer very seriously. A young boy died in the United States, an oral health care system very similar to ours.
His name was Diamante Driver, and his death, which was very unfortunate, has led to significant public policy interventions in the U .S. and Canada. We haven’t had a death in children. We have had deaths among the homeless, for example, but they don’t tend to receive a lot of attention.
And we also have tragedies like Mr. Moses Hahn here, who went blind in his eye because he wasn’t able to afford a root canal. Small business owner fell right through a specific crack in our oral health care system, meaning he was working poor.
So he made enough money not to qualify for public programs, but didn’t have the type of job that gave him employer -sponsored benefits. Again, one of the targets of the new federal dental care plan. Okay, so there is a tension in our culture because dentistry is health care, so it’s tasked to meet the needs of everybody in society, especially those that experience social and economic vulnerabilities that really is not up for debate regardless of how often I hear that dentists want to debate that fact.
And at the same time, you have the reality of dentistry today, which is far more business oriented than it’s ever been. And I’m not saying that that is a bad thing on face value, but it does create some public policy tensions and some cultural tensions within our profession and more broadly, that we really, really must address.
And if you’ve heard me speak before, you know that I spend a lot of time talking about this, because I do think it is important and probably incredibly consequential, or I would argue, incredibly consequential to us as a profession.
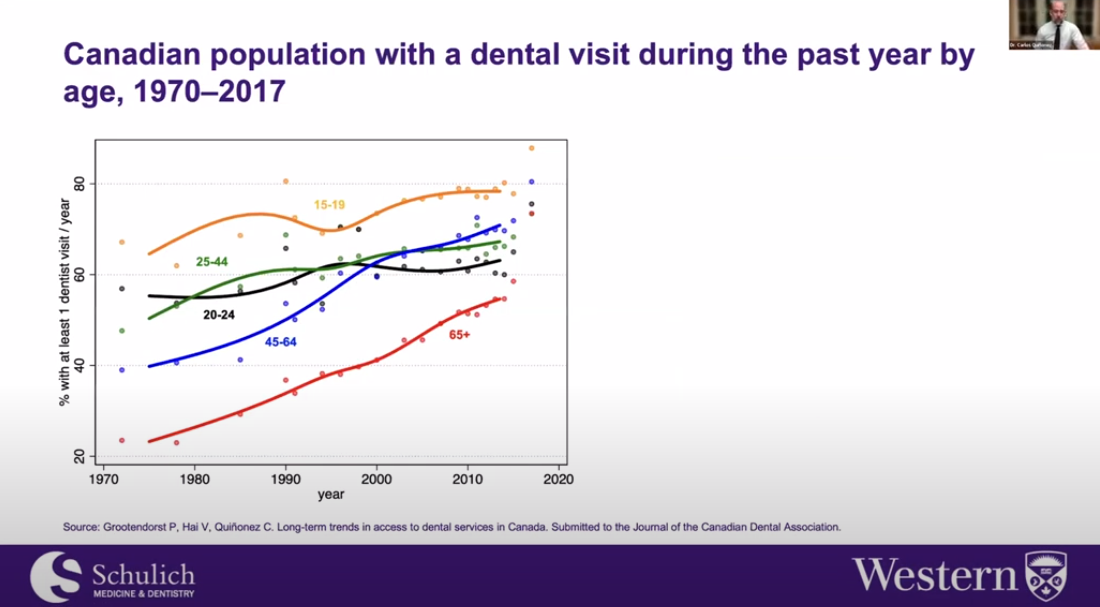
Okay, let’s pivot a little bit here and look at how people have been utilizing dental care from about 1970 to 2017. And you can see that over time, people have just been visiting us more than ever and that’s a great thing.
But why I want to show you this is because this is a signal that the public values what we provide them so much, that this is now and when they start having problems accessing what they value, among the electorate, there comes this public policy push, or it creates this public policy push, because a political dynamic is created that people say, no, we should have access to this.
And it shouldn’t completely depend on people’s ability to pay, which tends to be the way the system is structured right now. You should think about this not as a utilization graph but a political graph, the political importance of dealing with dentistry, it has only increased over time, and I would argue is is only going to continue to increase.
And part of that is because what we’ve depended on or Canada has depended on for so long, is it’s starting to become a bit weaker, right, we depend on employer sponsored health benefits, and employers have been trying to control dental care costs through benefits carriers who undertake the process of paying claims and so on.
And now our private dental care system, at least from the point of view of how it’s financed, is not as robust as it has been in the past. Again, contributing to this greater political interest in dentistry as people are finding it harder and harder to access care.

So much so that if you open up trade magazines today and in the benefits carrier industry, you’re going to see a lot of this, this idea that we somehow need to do something with respect to dentistry, you know, they pay for a lot so they’re very interested in the costs.
But you know, I want you to sort of keep this in mind because it will feature prominently with respect to the public policy issues that I would argue require attention.
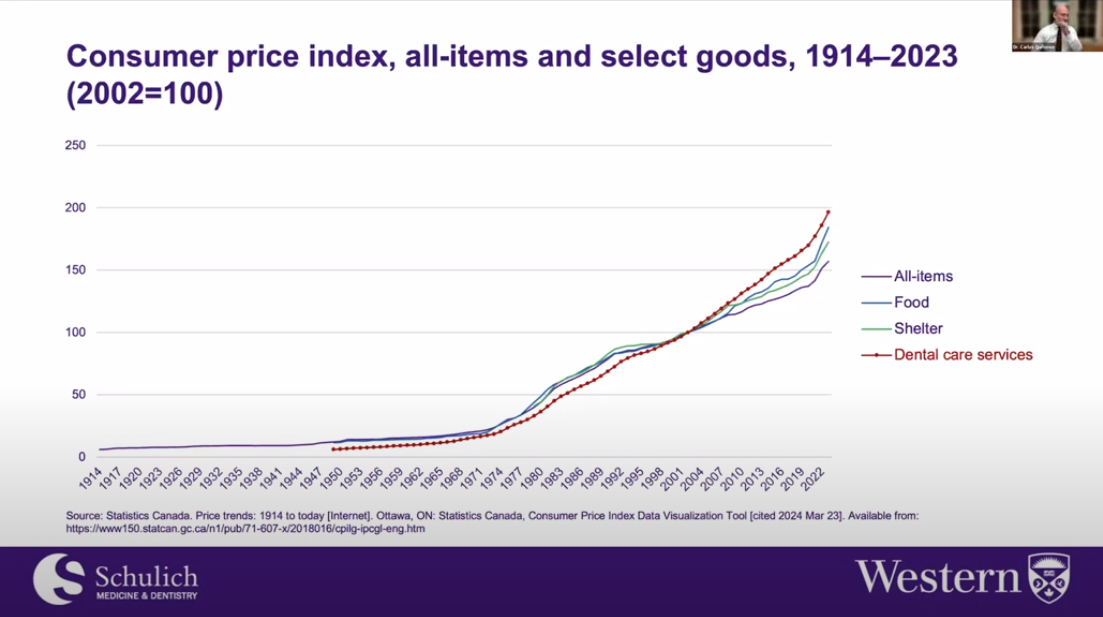
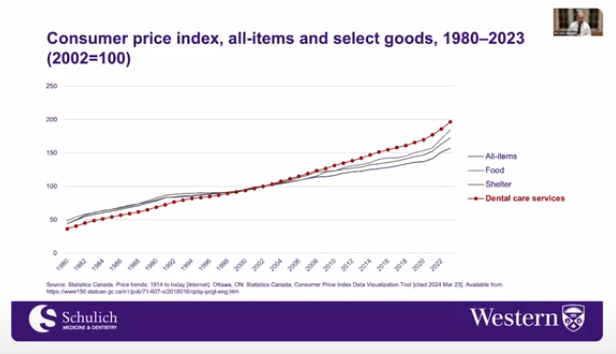
And if we just look at the consumer price index, you know, in a relative sense, we were more affordable than than all goods and services.
But in about the early 2000s, the increase in our in the pricing of dental care, the prices of dental care, our fees essentially started to outstrip all goods and services. And I’ve included shelter costs here because we’re hearing a lot about housing and the cost of that food.
We’re hearing a lot about that today. But we are more inflationary than than that. I’d like to also remind you that the federal dental care plan was was positioned as an as an affordability intervention, as this idea that that people, the average Canadian now needs some support, public support, communal support, if you want to talk about it that way, with respect to accessing care.
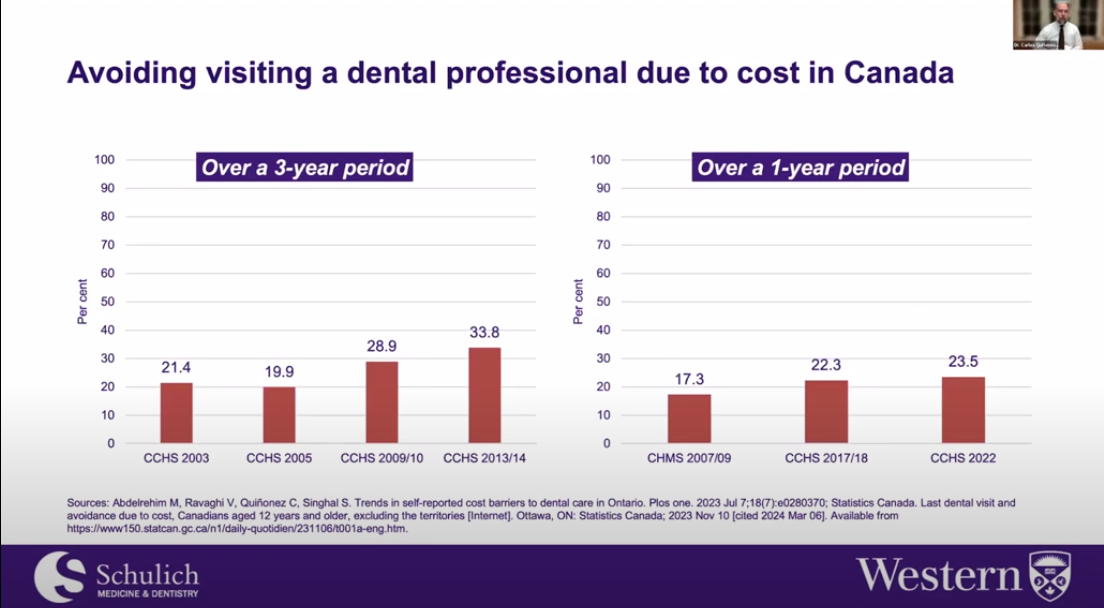
I saw Dr. Mona Abdel -Rahim, one of Sonica’s and myself former students, now a dental public health specialist in Alberta. She’s done wonderful work showing that access to dental care or avoiding visiting a dental professional due to cost has been steadily tracking upwards.
I include the latest data here from Statistics Canada and you know I’m not showing you all the data but we have data as far back in the mid -90s showing that year over year Canadians are reporting that it’s becoming more and more cost prohibitive to get to the dentist.
Again back to this idea that this is clearly has some political legs. I don’t want you to worry about any of these numbers but this and many other studies essentially are just tell us that the intervention to address cost barriers to dental care, the intervention to reduce differences in people’s ability to access care, at least in terms of income, is to provide public subsidies to be able to access that care.
It’s not telling people that they should brush and floss their teeth more, that they should eat healthier diets. Really if we want to shrink differences between the rich and poor in terms of being able to access care and even now the rich and the middle class, for example, we’re now seeing challenges even at those income levels.
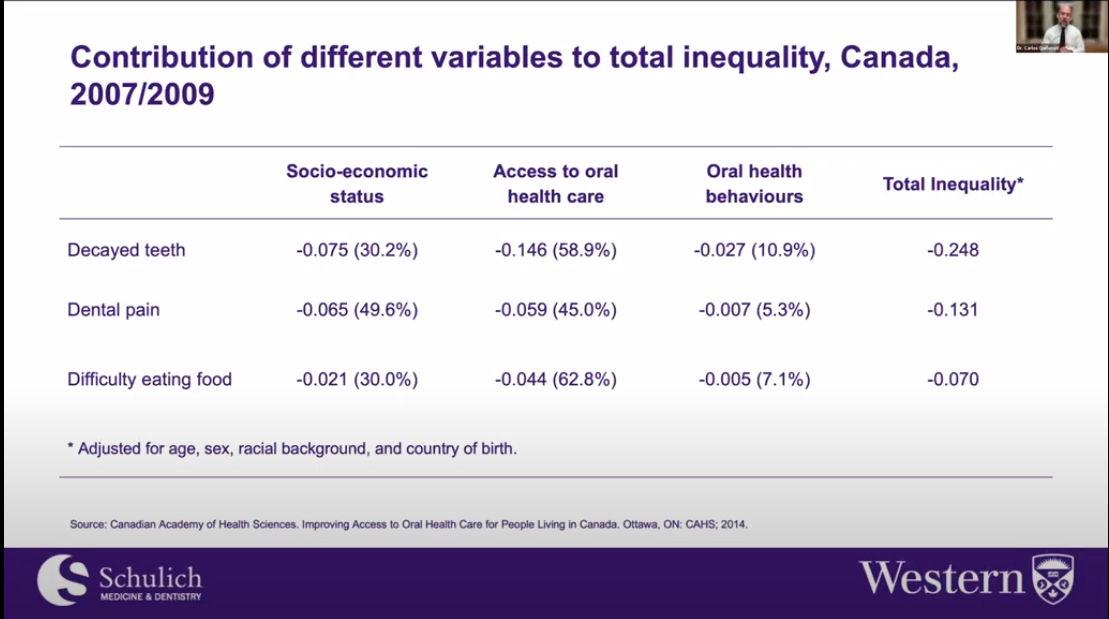
That’s why the federal dental care plan reaches up to a $90 ,000 income threshold. You know the intervention is what the federal dental care plan is which is a public subsidy to be able to remove the cost barrier to dental care and sadly I still hear from dentists that we should not do that, that the public policy intervention should really be about improving oral hygiene behaviors and don’t even get me started on that to a large extent.
I think that’s just victim blaming and scapegoating and we can debate that and I debate that with with Sonica and others in dental public health all the time but to me based on the evidence as I read it and not just this work by the Canadian Academy of Health Sciences but many other studies internationally with different populations, different countries shows that if you want to reduce inequity and access to dental care you provide people public subsidies so to me that’s not that’s not controversial.
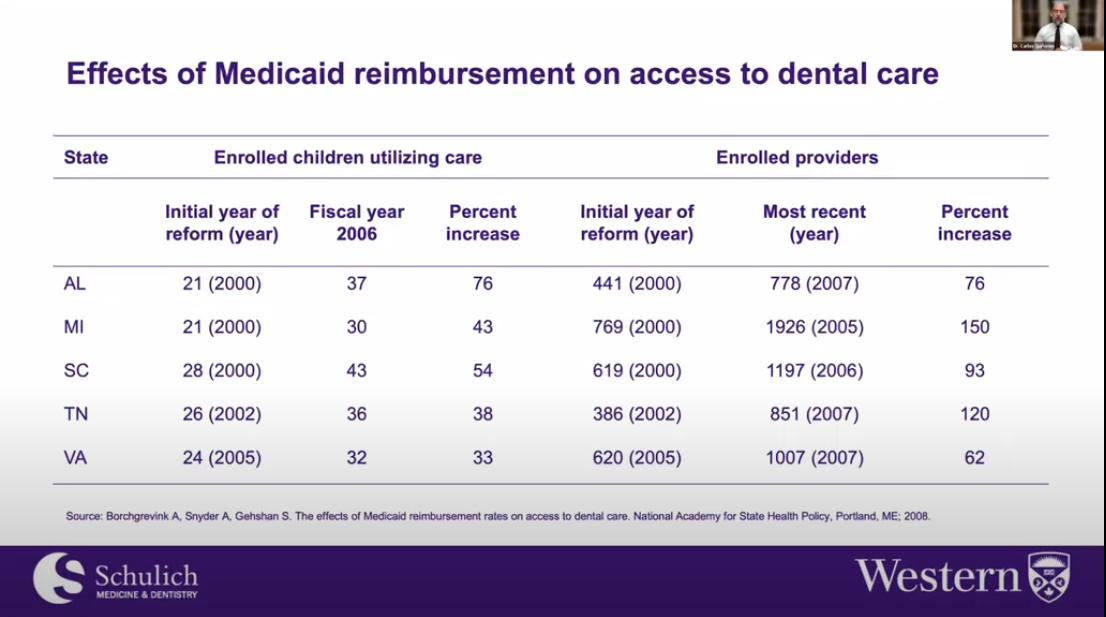
I also want to highlight the fact that what we pay dentists does matter. This is data from the United States that essentially again don’t worry about all these numbers just listen to what I’m saying if you can’t read the tables or graphs efficiently but this is just saying that if you increase you know public payment to providers they’re going to play ball, open their doors more more open the doors more more widely and more people are going to be able to access care.
So I think the issue of payment is not one that we can ignore but there’s a lot of nuance here and some things you you may not like to hear as I move on but I do want to acknowledge this because I think in places like my province Ontario dentists are dealt with incredibly unfairly you know 30 to 40 cents on what dentists suggested fee guides are is not an efficient way to engender provider acceptance of these plans and the patients that are covered by them but again a lot of nuance here.
What I do want to sort of highlight here, though, is that I think to some extent, we have focused far too much on fees in public dental care programs. I’m not saying it’s not important, but I think it really does send the wrong message to patients, to the public and ultimately to those in government.
And at least in my province, for a long time, we’ve become just totally, wholly focused on fees. One of my dearest colleagues in dentistry has long argued that we must divorce the idea of public payment from public policy discussions on access to care because focusing too much on fees is incredibly erosive to us professionally, and I would tend to agree, regardless of how horrible it feels to be treated so unfairly.
We have to control that part of our brains and focus on I guess the better angels of our professional nature, if I could put it that way. I’ll pivot to this notion of commercialism and dentistry because we have to do something about this.
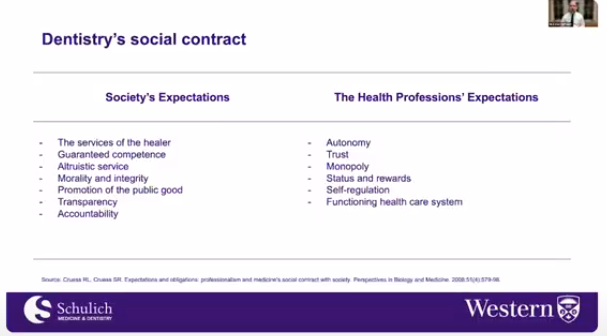
Why? Because it’s, again, not in line with what’s expected of us from society. Listen, we are part of a social contract with society. It gives us many, many benefits. It’s the status. It gives us the ability to generate a very good income.
It’s the basis of our professionalism. It’s why we are a regulated health profession. And when we just focus on money, on the business aspects of what we do, we erode or we send signals that we are not taking this contract as seriously as we should.
And I recently heard a story about somebody heard at a meeting, a dentist say, and I’ve heard this too, you know, I don’t remember signing a contract. Well, even though the social contract is unwritten, you know, there’s nothing you sign at all.
I’d argue that you did. When you signed for your license, you committed to what society expects of you. And we’ve collected data on what dentists think about these things. And unfortunately, dentists tend to disagree with many of the things that are expected of us through this social contract.
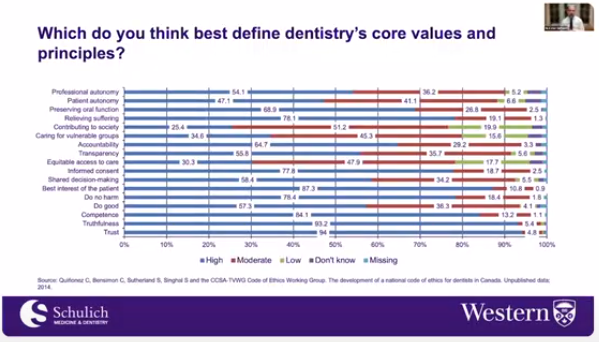
Again, this may be hard to see, but just things like doing good, 57 .3% of dentists are in high agreement that this is a core value and principle in dentistry. You know, that’s, that’s, you learned that in dental school, that’s called beneficence, a classic bioethical principle to do no harm.
78 .4% of dentists are in agreement that this defines dentistry’s core values and principles. Equitable access to care, the thing that we’re talking about today, to a large extent, 30 .3% of dentists are in high agreement, which means that a whole other two thirds are not contributing to society.
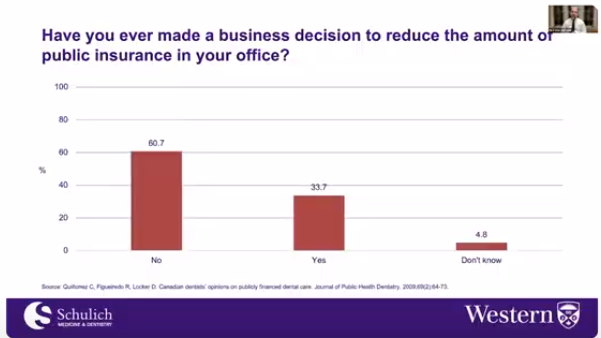
25 .4% of dentists are in high agreement. So clearly, you know, and again, if you heard me speak before, I’m not shy about this, we really need to correct this type of thinking. And ultimately, it does, it does hit our practices where we just are saying for for business reasons, we will not accept publicly insured patients.
And this is something that I would argue and have argued for a long time is very, very dangerous for us professionally and I’ll make that case as we move forward.
Now, a whole host of dental care policy issues were alive and well pre COVID -19.
I’m just listing some of them here that come to mind.
You know, take a quick look. But then COVID -19 hit and oh boy, oh boy, we were reduced, I would argue to two major public policy issues our infection prevention and control regime, and then a question of what actually is essential dental care.
I’m not going to get into the first one today. But I do want to concentrate a little bit on essential dental care, right, you know, as governments we’re, we’re, we’re starting to limit activities in society.
You got to be involved in health care, if you were considered essential as well as my and as one of my good colleagues reminded me recently, you know, we should never forget that early on, at least in our province in Ontario, and I don’t and I’m not sure about elsewhere.
But dentistry was not considered essential that should have sent us a very, very big signal that we have veered off the healthcare track maybe a bit too much because clearly we are essential. Now you thought COVID -19 was significant.
This to me are some of the implications, some of the more important implications of the new federal dental care plan. I’m just going to give you a little bit or a moment to to just take a look at this because I do think they matter.
Okay, so I’m going to group them into this. So these are what I believe to be the major public policy issues that require attention from all stakeholders. And I’m going to concentrate lots on on the dental profession, obviously, because that’s what we’re that’s who’s here today.
So we’ll go through one by one.
So the conflation of public and private spaces. So what do I mean by this? I think everybody appears to be confused between, you know, what an employer sponsored health benefit plan is and what a public health program is.
And that causes us a lot of problems in terms of efficient movement forward in the context of public policy. This is not new. This was recognized by the auditor general with respect to the non -insured health benefits program, you know, the NHB program, without getting into too much detail, the auditor general asked like, what is it?
Is it an insurance plan or is it a public health program? Because if it was a public health program, it would be thinking about itself in these ways versus if it was an insurance plan, which it appears to be functioning that way, according to the auditor general.
You know, is it that? And unfortunately, depending on who you ask on what day, it tends to be a little bit of both. And that’s fine. I’m fine with that. There are such things as public health insurance plans, if I could conflate the two.
But sometimes, again, it does not lead to clear thinking about why we do certain things. And I’ll get to that. Most recently, in INAN, the Standing Committee on Indigenous and Northern Affairs, which heard from the Canadian Dental Association, heard from Indigenous advocates, Indigenous groups, and so on.
And a recommendation was made that to me, I think shows how confused we have become that the non -insured health benefits program, in order to ensure that cover that it needs to ensure that coverage for procedures is comparable to other dental programs, such as the Federal Public Service Dental Care Plan.
No, no, no, no. NIHB is a public health program. So why are you asking that it looks like a private dental care plan that essentially is born out of labor relations, right? Those two things are very different.
And unfortunately, I think dentists and governments are trying to stick public health programs or public health dental care plans into the model of an employer -sponsored benefit plan. And it just causes way too many challenges professionally, from a policy perspective, politically, and so on.
Now, the reality, though, is that dentists prefer this. To some extent, governments prefer this. Why? Well, we know that there’s less administration with private plans. We know that they pay us at fees that we are more comfortable with.
But the reality is that the accountabilities for a public health plan are different. The oversight is different, simply different than an employer -sponsored benefit plan. Okay, what about low -value dental services?
Well, we want to push services into public service schedules that support our business model, but do little to support individual and population health. There are now open questions about the therapeutic value of some dental care.
And this is a type of dental care we want governments to fund. This does not make sense. So I’ll make my case.
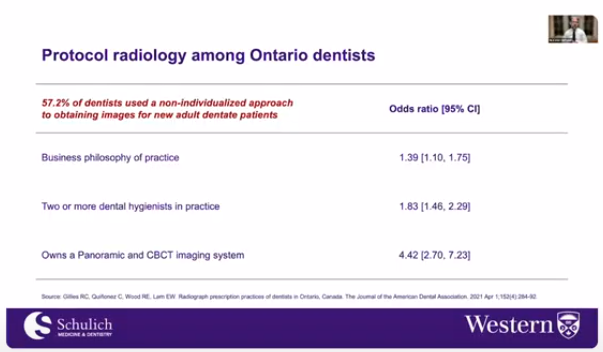
Things like unfettered diagnostics. This is the work of Roland Gillies, former, or radiology resident that I was lucky enough to work with, that showed that 57 .2 percent of dentists in Ontario use non -individualized approaches to radiographs, essentially protocol radiology.
So as opposed to prescription radiology, which is what we’re supposed to do. And if you were a dentist that reported more business philosophy of practice, you were at a higher risk of being or undertaking protocol radiology as opposed to prescription radiology.
If you reported owning a panoramic x -ray machine or CBCT, you were at a very higher 4 .4 times higher likelihood of engaging in protocol radiology. Again, I understand why that makes sense from a business perspective, but definitely not from the point of view of evidence -based care.
And we do the same thing with things like unfettered prevention, arguing that government should pay for things like oral hygiene instruction. Listen, you don’t need to be a rocket scientist to know that five minutes a year with a dentist or even half an hour with a dental hygienist somehow is going to radically change people’s oral hygiene behaviors.
Health behaviors simply don’t change that way. It’s far more complex. There are whole schools or divisions in public health schools that are trying to unravel the mystery of health behavior change and they’ve been at it for 100 years.
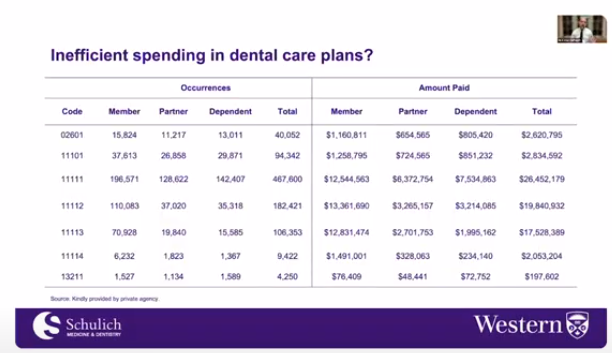
We definitely don’t have the answer to that, so why would we expect governments to pay for that? This is data from a private insurance plan that shows that some private insurance plans are still paying for this.
To me, this is money just going down the drain and when it comes to tax money, again, why would we ask this? What about routine scaling and polish? Now, I’m starting to get very controversial here, but the evidence is increasingly clear.
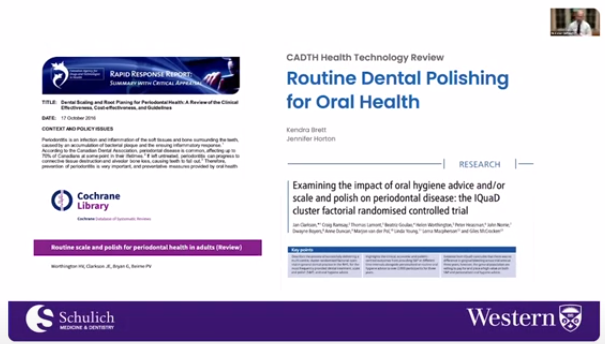
Oral hygiene instruction and routine scaling and polish do not add anything to individual and population health. The latter are nonetheless asked by the oral health care professions. Dentistry, dental hygiene come to mind with respect to demanding that governments pay for this.
Now, what is important about some of the most recent data is that things like routine scaling and polishing is very valued by patients. I want you to keep this in mind as it will become important shortly.
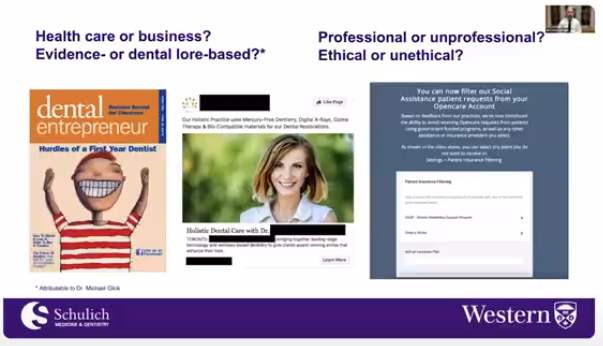
Okay, the next public policy issue, health care versus the business model of care and dentistry. Again, I believe we really need to pay attention to this. Here, I just want to highlight the notion of what is health care and what is body work.
That’s a sociological term for things that make you feel better, but don’t necessarily have major impacts on your health. I’ve heard it spoken about quite disparagingly, sort of health care versus haircuts.
I’m starting to talk about it more as wellness versus health care. But again, the issue is what is medically necessary or essential dental care? And the reality is that we’re being questioned with respect to that.
This is from the Atlantic. It’s now a bit of a famous piece, but you see this popping up all the time in media. Dentistry is much less scientific than you think, more prone to gratuitous procedures than you may think, and private insurers are now also starting to ask very, very similar questions.
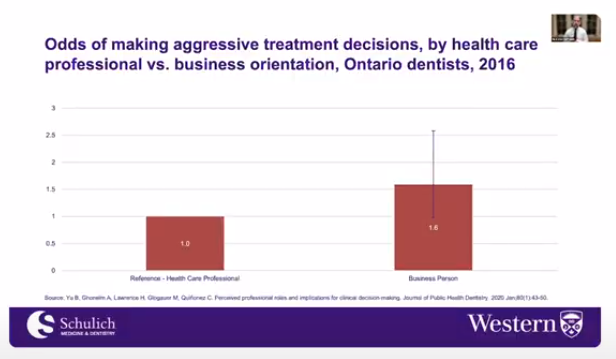
And the reality is that those things prop up the business reality of dentistry, but that can be damaging to our patients. We’ve done research to show that if you’re a dentist who is more inclined to business, you are at a higher likelihood of making more aggressive treatment decisions.
This is well documented in medicine with surgery services, and here’s some data from us with respect to dentistry. So then this is the latest. Phrenectomies appear to be all the rage. I’ve reviewed the evidence of therapeutic benefit, and it’s lacking.
There is some benefit, but it’s very short term from what I’ve read, and definitely no long -term studies here. And the outcomes can be very, serious, and we are running with this from a business perspective, but really, should we be doing this?
I would argue no, and I know that can be controversial, but there you go. Providing evidence -informed care is incredibly important. It’s part of the social contract, actually. It’s the basis of healthcare professionalism to some extent as well, and the more we lean into the reality of business, the less steady the professional ground becomes, maybe even a slippery slope.
And we have to ask ourselves some very hard questions here. As one leader described to me recently, the reality is that the profession has split. There are oral health care professionals, and then there are people involved.
And this is simplistic, but just take it for what it is. People involved in cosmetic dentistry. Now, that’s a bit of a tautology. Name me a part of dentistry that doesn’t have some aesthetic component to it.
Nonetheless, this is the picture my colleague was painting. You know, they said that today the average practice has a hygiene mill for base revenue, with the dentist working on relatively healthy people, selling them high -end services.
Now, these are not my words. I’m just giving you a sense of what is being said. So I’d argue that we need to think about this very closely. Could it be that our current model of practice is not suitable as a primary care environment?
So let’s move to the next public policy issue, scientifically and ethically defensible resource allocation and priority setting. Now, I know that that sounds like a lot, but I use the previous term primary care very strategically here, because we are part of the primary care system and we must not forget that.
And resource allocation and priority setting is just the more modern way of saying how should we ration dental care?
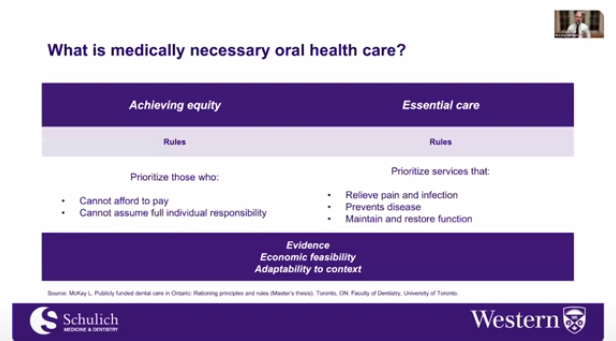
We’ve done some work on this. This is the work of Linda McKay. Where she showed that a stakeholder said that essential dental care, relief pain and infection prevented disease and maintained and restored function.
That’s great, incredibly clear and cogent, but what services can we attach to that?
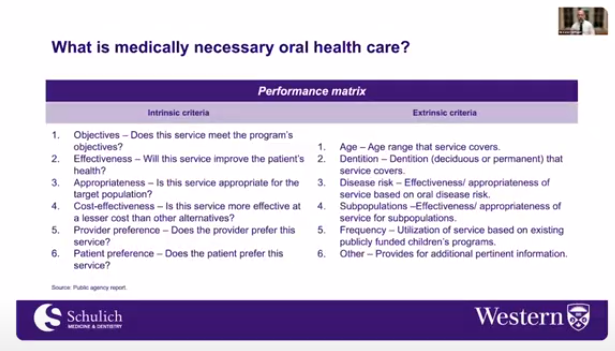
Here, I can’t share details, but we’ve been involved in taking very technocratic approaches to trying to figure out what service matches that definition.
And again, I don’t wanna provide any details, but this is the type of work that we must do in order to achieve scientifically and ethically defensible resource allocation and priority setting. So a related question is what should be in a primary dental care basket?
And who decides? Well, again, this is the domain of resource allocation and priority setting, or more specifically, resource allocation ethics. And best practice in deciding what should be part of primary healthcare baskets is a deliberative one.
The days of doctor knows best are long gone. Other individuals must be involved in making decisions like the public with respect to what governments are gonna pay for, for example.
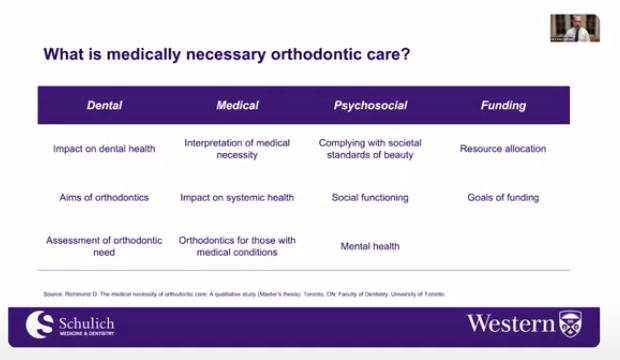
And here, I wanna point you to the wonderful work of Daniel Richmond.
And I saw he’s on the call tonight, a recent orthodontist grad who’s done some incredible work around what is medically necessary orthodontic care. And again, I’m not gonna get into the details, but what Daniel was able to show was that there are a variety of things that need to be considered with respect to medically necessary orthodontic care.
There is some argument to be made that some of this should be covered by governments, but what you need is a process of deliberation in order to be able to make this decision in an ethically and scientifically defensible way.
Because there is ultimately too much scientific and moral controversy in these types of questions. And what’s good for us here is that, as my colleague reminded me, this provides us with new possibilities for ethically meeting patient care needs by connecting what we do to broader psychosocial and societal outcomes.
You know, we matter. And there’s avenues for us to explore here, but just saying that we should cover diagnostics with no oversight or scaling and root plannin replaining with no oversight, you know, we cannot lie to ourselves and to others.
That’s just, from my perspective, inappropriate.
And the non -assured health benefits actually has an oral health advisory committee that makes recommendations to, for example, what might be covered.
It’s just advice. It’s not binding, binding in any way, but it’s an independent advisory body. And it meets best practice and resource allocation ethics. And my sense is that we would see something similar with the federal dental care plan.
And, you know, there’s nobody from the associations here, there’s nobody from industry. It’s impartial advice as best as possible.
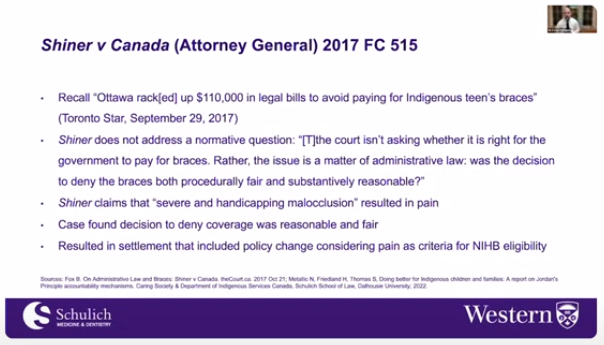
And these processes matter because when governments get involved in paying for care, some people say I’ve been treated unfairly.
In the NIHB, one of the individuals they covered said, you know, you’re not treating me fairly by not covering my orthodontic care. And it went to court. And this is really important. The court ruled that it wasn’t a decision of whether the individual needed the orthodontic care or not, but it was an issue of administrative law, was the decision to deny the braces both procedurally fair and substantially reasonable.
That’s why you need these deliberative processes. And I know we’re short on time, so I’m going to move a bit more, a bit more quickly. Now to some really controversial stuff, the pricing of dental care.
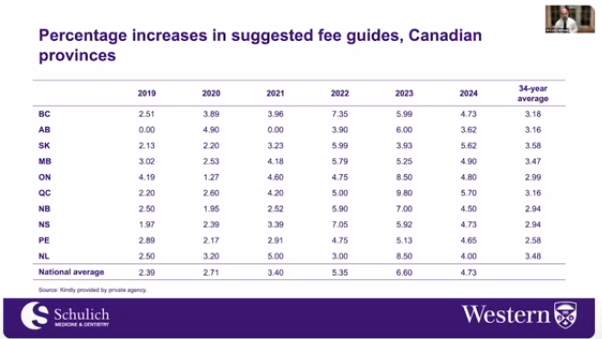
These debates have been popping up over time, most recently in Alberta, where they actually had to introduce a service schedule. And, you know, this has been something that we have taken a little bit in terms of a comparative approach with the federal government.
And I would argue that that combative approach is inviting close and potentially uncomfortable scrutiny in terms of how we set fees as a profession. I would also argue that we will not curry favor from the public with concerns over what we perceive as fair remuneration.
What is fair? Now, according to a good colleague of mine, who’s a dentist and also a business professor at a major university, he argues that it’s at 87 .5% of his provincial suggested fee guide. I don’t know, but I can tell you that it’s not 100%, okay?
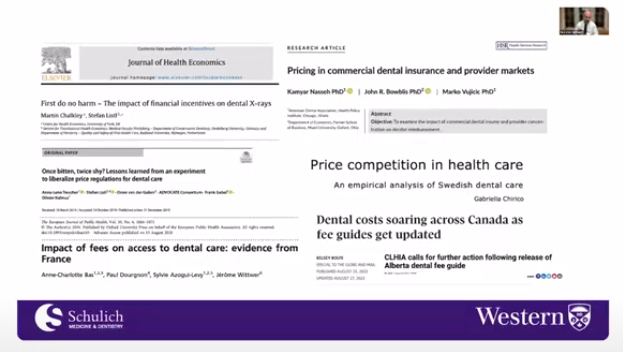
And there’s increasing empirical investigations and media attention on the pricing of dental care and its implications, and we will not escape this. I think we need to pay very close attention to this.
And I know this hits us, you know, where it can get very uncomfortable, but we cannot ignore these things.
In fact, we’re now seeing the beginnings of price competition in the Canadian dental care market, specifically in Ontario and maybe elsewhere.
So this combative stance of ours with the federal government, you know, I want to remind you that governments and politicians of all stripes are much closer to each other than you think. They pay attention to what each other is experiencing and perception counts.
There is a perception, unfortunately, that dentists are acting as business people first, and we are fueling that perspective. We are not business people first. We are health care professionals first, and pushing the business agenda is, to me, a very efficient road to professional ruin.
I know that sounds intense, but I do mean it. At best, we are damaging our future engagement with governments and the public. So I ask you, as an industry, is this pricing agenda sustainable?
We’re almost done.
we I would argue that we have an underdeveloped or unevolved or unfortunately unsophisticated policy perspective. The arguments that we’re providing to governments from my perspective are things that we’ve been saying to governments since the early 1900s, individual choice, the sacrosanctity of the clinician -patient relationship, the therapeutic value of unfettered diagnostics and preventions.
You know, here I want to pay attention to the reaction that we’ve provided the federal government with respect to its claims processing and payment agreement. Now I don’t have time to get into the nuances here.
I know that it’s not what we normally accept, but the reality is that much of what it’s saying is standard. Keeping claims documentation for two years as part of regulation, recovery of funds in the case of overpayment, that happens all the time with private payers.
On -site audits involving provincial regulatory bodies, that’s been happening for well over 15 years now. As well as a colleague recently reminded me, what the billing agreement says is often in our public programs, provincial public programs, structured into legislation, regulation and policy so we don’t see it, so we don’t think about it, but once it’s in front of us, but these things occur as well in the private sector.
So if this is the case, what exactly are we fighting against? I think it’s an issue of ideology. What we believe is true, what we value, but unfortunately we are not convincing from the point of view of evidence, let alone when viewed against more contemporary policy perspectives on health care.
We must evolve, we must become more agile.
Okay, dentistry’s governance. I would argue that the federal government miscalculated in dealing with the Canadian Dental Association early on. Dental federalism is unique.
Provincial and territorial dental associations are very important to the politics of dentistry in this country, but the reality though is that certain things are done in certain ways in Canadian Confederation.
So in that sense, I would argue that the profession also miscalculated. I would argue that we have weakened our national strength and presence by becoming too provincial. I also want to highlight the fact that in those provinces where you’re both an association or regulator, this could be very damaging.
We’re reflecting a union mentality when we’re supposed to be acting in the public interest. We must put the oral health of Canadians first and our associations appear to be putting the economics of their members first.
And when combined with the issue of pricing, all this has the potential to become incendiary for us. And lastly, professionalism and access to care, like why are you ending with this, Carlos? Well, I think some of the greatest risks here remain.

The federal dental care plan will not solve our access to care issues. In fact, it may create others. As a regulated health profession, we are tasked with helping to address this issue and the perception, rightly or wrongly, is that we don’t care as much as we should or care as much as society mandates us to.
The federal plan is just one intervention. There will be other interventions if we do not address this issue. Again, I’m thinking about the long game here. One of my closest colleagues said that this is actually not about fees.
This is about fearing the loss of professional control and autonomy. And I would argue that if these are our fears and our approach as individual dentists and as a collective today will only incentivize more public policy intervention moving forward.
Thank you very much.
Thank you. Thank you so much, Carlos. I think it was so amazing providing a comprehensive overview of the Canadian oral healthcare system. And also, you know, providing history of it that why we are here, where we are.
So that really helps with all the history, you know, you also shared. So thank you so much. So as we are waiting, people can type in their questions in the Q &A section as Dr. Zard mentioned earlier.
And…
I can jump in if you like, Sonika. We have a question, Carlos. First of all, Carlos, thank you so much. You’ve given us a lot to think about, a lot to discuss. We just obviously need for further discussion on this really important area and really appreciate your insight, your take.
I think this is invaluable information for our community to really ponder on very seriously. So thank you. We have a question from Dr. Lauren Chapnick. Lauren says, you said that an Ontario dentist are not being fairly compensated.
The question is, does the government program compensate dentists adequately?
So if the question is, does the federal government program compenstate dentists adequately? Well, this is my opinion as a public health dentist. 80% of provincial suggested fee guides, to me, is fair.
In fact, at a certain point, we were arguing that we just needed to be paid 70%. But then over time, the goalposts have moved, and now people are saying, no, we need to get paid 90%, 100%. I’ve even heard 120%.
More formally, though, I don’t know whether it’s fair or unfair. That is for us to discuss with the public, to discuss with society. And unfortunately, I think dentists think that that conversation is only for us to address.
And the reality is that in today’s broader health care policy environment, again, the idea that dentists knows best, those days are gone.
Thank you. I have a question from Dr. Michael McIntee from British Columbia. How would you anticipate that the dental profession would lose its autonomy?
Well, if we don’t address these issues, I would argue that eventually government is going to turn to regulators and say you’re going to have to regulate more heavily. You know, as an example, you will have no choice.
You will have to see all patients.
That’s a sobering thought. Thank you. Are there any other questions? So we’ve run a little bit over. Hold on. We have one more question here from Pierre Eric Laundrie. Canada is not the first country to tackle national dental health, cost, and accessibility.
How do the best have or are handling the issue? And how can we not? Why can we not copy, adapt, or adopt similar models?
Incredible question, Dr. Landry. And I think we need to look internationally to see what is best practice. You know, I always like to talk about the German system. But if you go to Germany, they say, Oh, my God, we have so many problems.
But it’s really perspective, right? They have some of the smallest differences between income groups in terms of access to dental care, they spend, you know, dentists make lots of money, if I can be cynical, you know, they have some of the best oral health statuses in the world, in an average sense.
And, you know, there’s good stuff going on in the Netherlands, there’s good stuff going on in the US, there’s good stuff going on in the global south, I think we just need to look.
Thank you. We have one other question from British Columbia from Dr. Peter Stevenson Moore. Thank you for discussing the importance of oral health versus the importance of dentistry. Why does government concentrate on getting money out of the door as opposed to defining what the problem is and then working on the best use of funding and resources to address the problem?
So Dr. Stevenson Moore, I wish you were in charge. Now here I will cut my federal colleagues some slack and in fact say that the NDP have really pushed the agenda far too quickly. I understand why politically they would wanna do that, but you don’t stand up a national dental care plan in the time that the federal government has been given.
I mean, you do that, but then you have to deal with the challenges that are created during and then post -Hawk. I think we will deal with those challenges and those problems moving forward. But I think our current government has been treated a little bit unfairly because of the desire of the NDP to just get this going.
I think if they would have done things or been given the time to do things like appropriate problem identification, I think we would be in a better spot than we are today. But given the timeline, this is where we are and there you have it.
Thank you. Dr. Michael Glaughauer, is this dental finding program a gateway to two -tier healthcare in general? Is dentistry in fact the savior of healthcare period?
Yeah, so Dr. Glogar and I talk about this all the time. I would argue that we already have a two tier dental care system, maybe even a triple tier. We already have a two tier healthcare system. This may sound horrible, but one of my very good colleagues told me once that, you know, there’s the healthcare system in Canada that exists for the prime minister.
There’s the one that exists for the hockey players. There’s the ones that exist for the healthcare professionals like us. And then there’s the one that exists for everybody else. You know, that’s a joke, but the reality is that people have different resources in their ability to access healthcare.
So we do have a little bit of that tearing going on. Now, do I think medicine can learn from dentistry? Yes, I do think so. Medicine has many of the same issues, you know, paying for things that don’t, that we shouldn’t pay for from the point of view of the public purse, allowing certain things to enter the private sector.
Listen, this idea that dentists have that this federal dental care plan is the thin edge of the wedge and it’s all be part of Medicare. There is no country internationally that has a single payer dental care system.
So why would we do that? We have mixed systems of funding, financing, mixed systems of delivery. That is the future of healthcare internationally, whether it’s dentistry or medicine.
Thank you. Are there any other questions? We’ve gone a little bit over, but we still have time maybe for one or two more. A question from Terry Farkar. There is a trust issue, I think, with government intervention and the desire for votes.
Can we discuss also if overhead is 70% to 30% decrease in fees, is 100% decrease in income from the provider?
So Dr. Farquhar, I agree with you, there is a trust issue and it goes in both directions. Now with respect to, you know, the 70% overhead, 30%, you know, listen, I think that’s too simplistic in terms of how we view dental practice, right?
At a certain point in the day, your fixed costs will be paid, you know, your variable costs will, you know, well, obviously don’t behave like fixed costs, but, you know, I always say that, you know, major retailers don’t sell their products at 100% of their fees.
They understand that there’s gonna have to be some level of discounting. And in fact, discount retailers, that’s how they make most of their money. You know, I’m not suggesting that dentists should be discount retailers, but, you know, not accepting 100% of your fee doesn’t need to be an economic drain for you.
In fact, you can, there are business arrangements that allow you to be just as successful economically based on what I’ve seen in other healthcare markets, for example.
Thank you. We have time for one more question. Anybody else out there? Thank you, Carlos. So you’ve obviously stimulated a lot of a lot of thought. I think there’ll be a lot of discussions tomorrow in different specialist offices and universities and research institutions across the country on this this topic, which continues to evolve in some pretty strong emotions, I think within within the community, understandably so.
So seeing none on behalf of the Fellowship of First Committee, I’d like to thank you, Carlos. Thank you so much for volunteering your time, sharing your expertise. I think this was this was terrific and much appreciate.
Thank you. Before we conclude tonight, we have some more polling questions. Kindly answer the questions that show up on your screen. And these questions tonight focus on upcoming events that the RCDC is involved in and our attempt to connect with you across the country.
For those of you aware, there’s the Canadian Health Summit being held in Halifax this June. The RCDC is hosting a networking event. Please join us if you happen to, if you’re planning to be at at this meeting, you’ll get information specific to this.
The second thing we’d like to get some feedback on is we’re starting a new initiative this summer. This was the idea of Dr. Sandy Vaduk from University from Vancouver. We’re planning these lunch and learn sessions for graduate dental specialty residents across Canada, with the RCDC being the responsible organization to administer both the NDSC and the fellowship exam.
We’d like to meet with new residents as they start and embark on their programs and giving them information about these two exams. We’re asking for you to help us out at your respective universities that are interested in volunteering.
And finally, and very importantly, our third annual sea event is taking place at the Empress Hotel in Victoria, British Columbia on Friday, September the 27th. This is our new tradition of having a day of sea followed by our AGM and our convocation of new fellows.
If you haven’t yet, please mark your calendars. Dr. Michael McEnteed, who’s on this webinar tonight, is our going to be giving our keynote address. Looking forward to that. And Dr. Mike Mallow has put together a wonderful program for us for the Friday.
So if you haven’t yet, take a look at your calendars and please consider joining us.
Dr. Tsar, there is one comment by Dr. Stephen Sennmoor and he’s asking, would the slide deck be shared?
I’d have to ask Dr. Gionis.
So just a quick answer to that, I can’t share all of it because some stuff is not for me to share, but just email me and I will share what I can.
Thank you, Carlos, that’s very kind. Thank you, Sonja. This concludes tonight’s session. Look forward to having you join us on April 30th for our last, sorry, for our next webinar. We’re returning to the theme we started last year.
We’re putting a spotlight on graduate specialty programs across the country. This time, we’re focusing on the graduate and the daunting program at the University of Toronto. We’re gonna have wonderful presentations from current residents and look forward to seeing you at that event.
Leave a Reply